The Problem
Treatments for chronic neuropathic pain are insufficient and the most effective options have high addiction and abuse risks.
Chronic Neuropathic Pain
Experiencing persistent or recurring pain for longer than three months (chronic) as a consequence of direct trauma to a nerve, such as a lesion or disease (neuropathic) is known as chronic neuropathic pain.
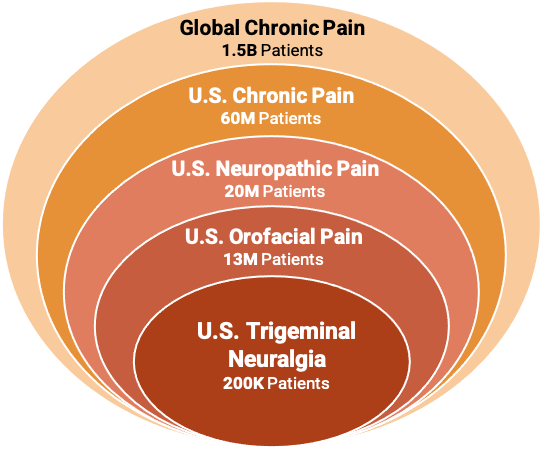
Chronic pain is the leading cause of disability and costs the U.S. $635 Billion annually.
Chronic pain affects more than sixty-million people in the United States, affecting more adults than heart disease, diabetes and cancer combined.
Neuropathy is the leading cause of chronic pain, affecting twenty-million chronic pain sufferers.
Neuropathic pain can occur locally near the nerve injury but can also spread to other areas due to the complex branching nature of neurons.
Trigeminal Neuralgia is a specific type of neuropathic pain.

Trigeminal Neuralgia
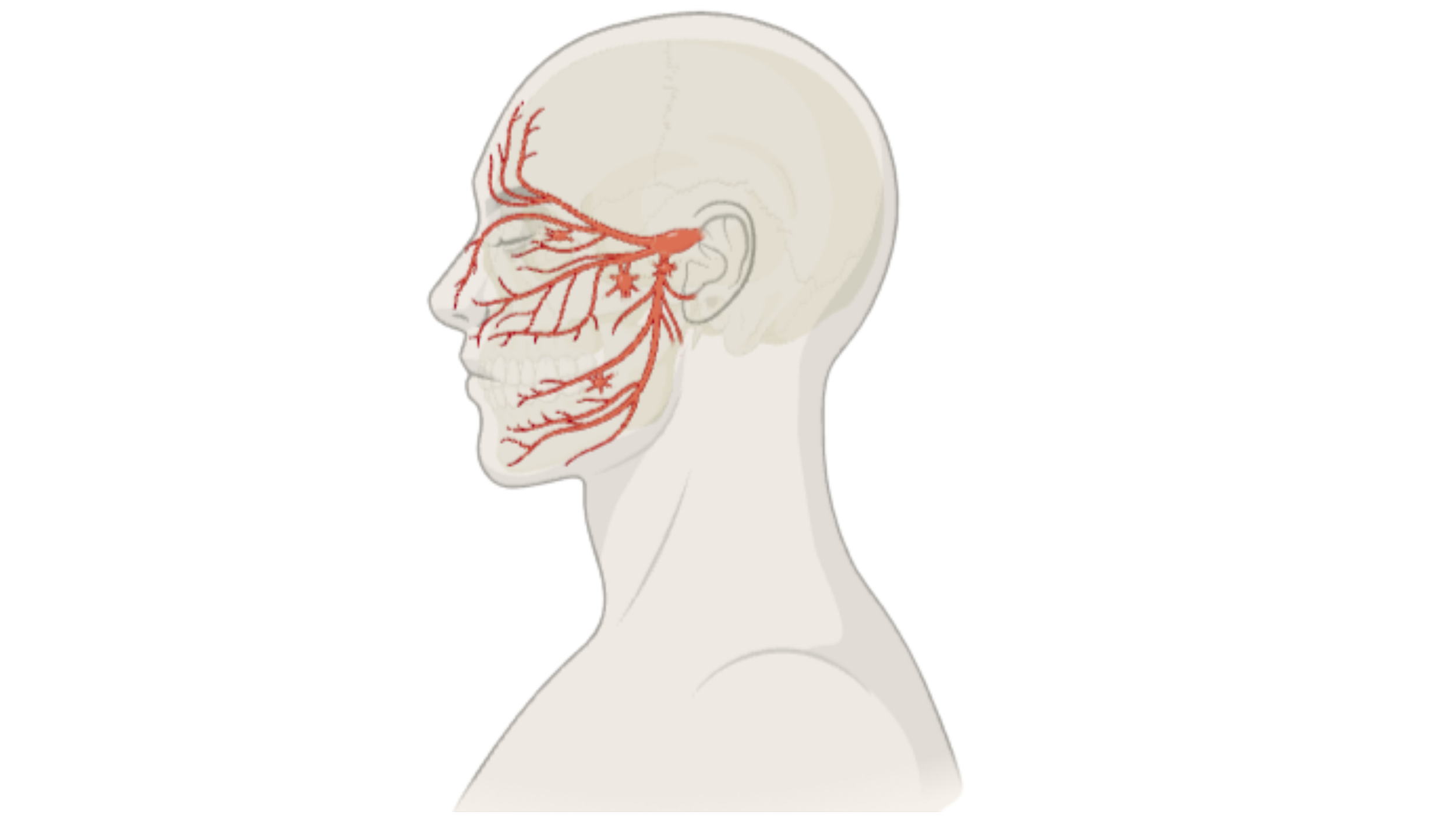
Trigeminal Neuralgia is a medical condition of the trigeminal nerve causing intense and debilitating facial pain with electrical shock-like spasms, often described as a severe stabbing pain in the face.
There is one trigeminal nerve on each side of the face that branches into three distinct nerves that provide sensory information throughout the face. They are primarily for sensory feedback, such as the feelings of touch, temperature and pain in the face, but also control the muscles needed for chewing.
While any of the branches of the nerve could be independently injured, trigeminal neuralgia can occur spontaneously with no known cause, or in response to damage, pressure or disease affecting the trigeminal nerve. When this nerve is affected, it can affect sensation in all three subsequent branches.
Trigeminal Neuralgia is most common in adults over fifty years old and is referred to as the “suicide disease” with approximately 25% of patients experiencing suicide-related thoughts or actions.
Treatment for trigeminal neuralgia remains poorly managed with current medications primarily targeting the symptoms but result an array of side effects or only offer modest relief. Surgical interventions can also be done, coming with their own unique set of risks and side effects.
What Causes Trigeminal Neuralgia?
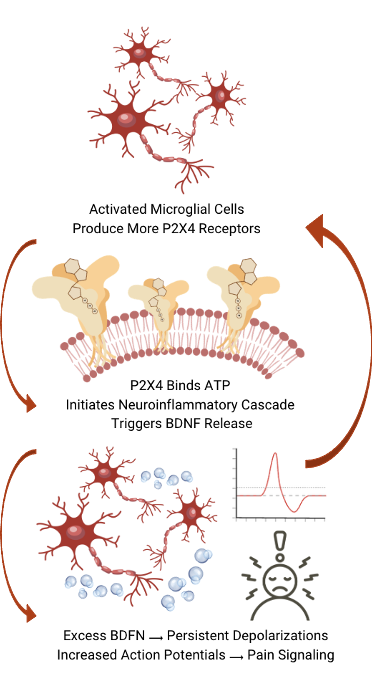
Damage to the trigeminal nerve by a lesion or disease activates an inflammatory response that becomes uncontrolled and cyclical.
Nerve injury actives microglial cells, which are immune cells for the central nervous system (CNS). These cells act as the first line of defense by detecting pathogens and cellular damage and initiating inflammation to protect the CNS. Upon activation they begin producing excess P2X4 receptors. These receptors bind to adenine triphosphate (ATP), initiating a neuroinflammatory cascade, triggering the release of Brain-Derived Neurotrophic Factor (BDFN).
At normal levels BDFN plays a key role in the survival and nerve regeneration, promoting axonal regrowth, and protecting neurons by enhancing DNA repair mechanisms. When too much BDFN is present it causes excessive calcium and sodium ions to fill the cell, resulting in depolarization of the cell. Once a neuron reaches a specific threshold of depolarization it with fire and send a signal, called an action potential.
In an ordinary nerve injury BDNF does not excessively accumulate, so this response isn’t seen. In Trigeminal Neuralgia, this excess BDNF continues to repeatedly depolarize the nerves, resulting in a chronic, repeating neuroinflammatory response and associated pain.

Treatments for Trigeminal Neuralgia
Surgical intervention can be done both indirectly (non-destructively) or directly (destructively).
Surgical interventions each have varying levels of success, invasiveness, and potential numbness. These procedures are not a candidate for patients who are unable to undergo anesthesia.
Non-destructive intervention is achieved by microvascular decompression, relieving pressure on the nerve from surrounding tissues, most often targeting an adjacent blood vessel. It is effective but requires invasive procedures.
Destructive intervention options as done by damaging the nerve or physically removing a portion of it to block the pain signals. These therapies include both invasive and non-invasive techniques with varying levels of success, invasiveness, and potential numbness.
Pharmaceutical treatments include antidepressants, gabapentinoids and opioids, each with varying levels of relief and side effects.
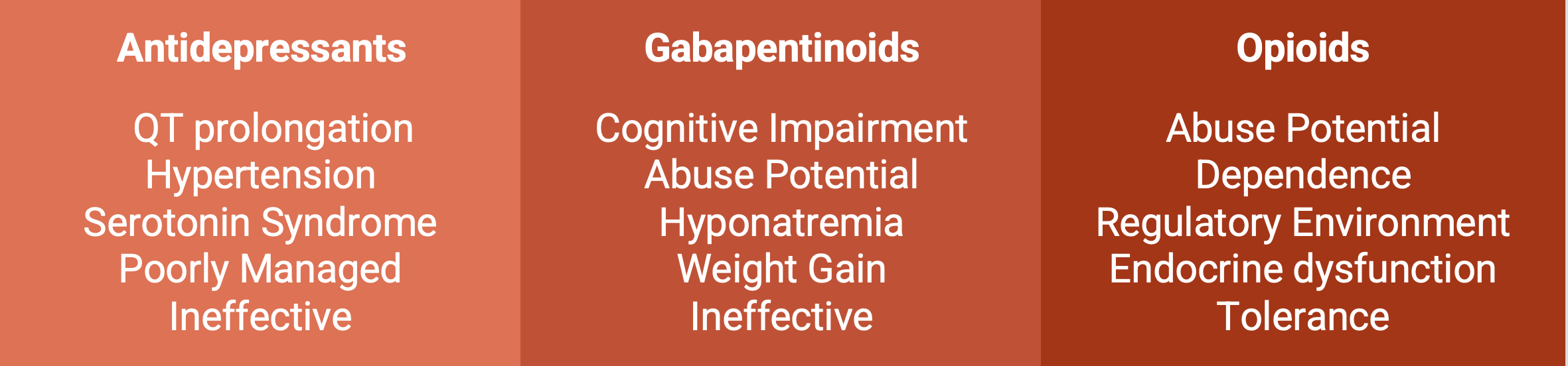
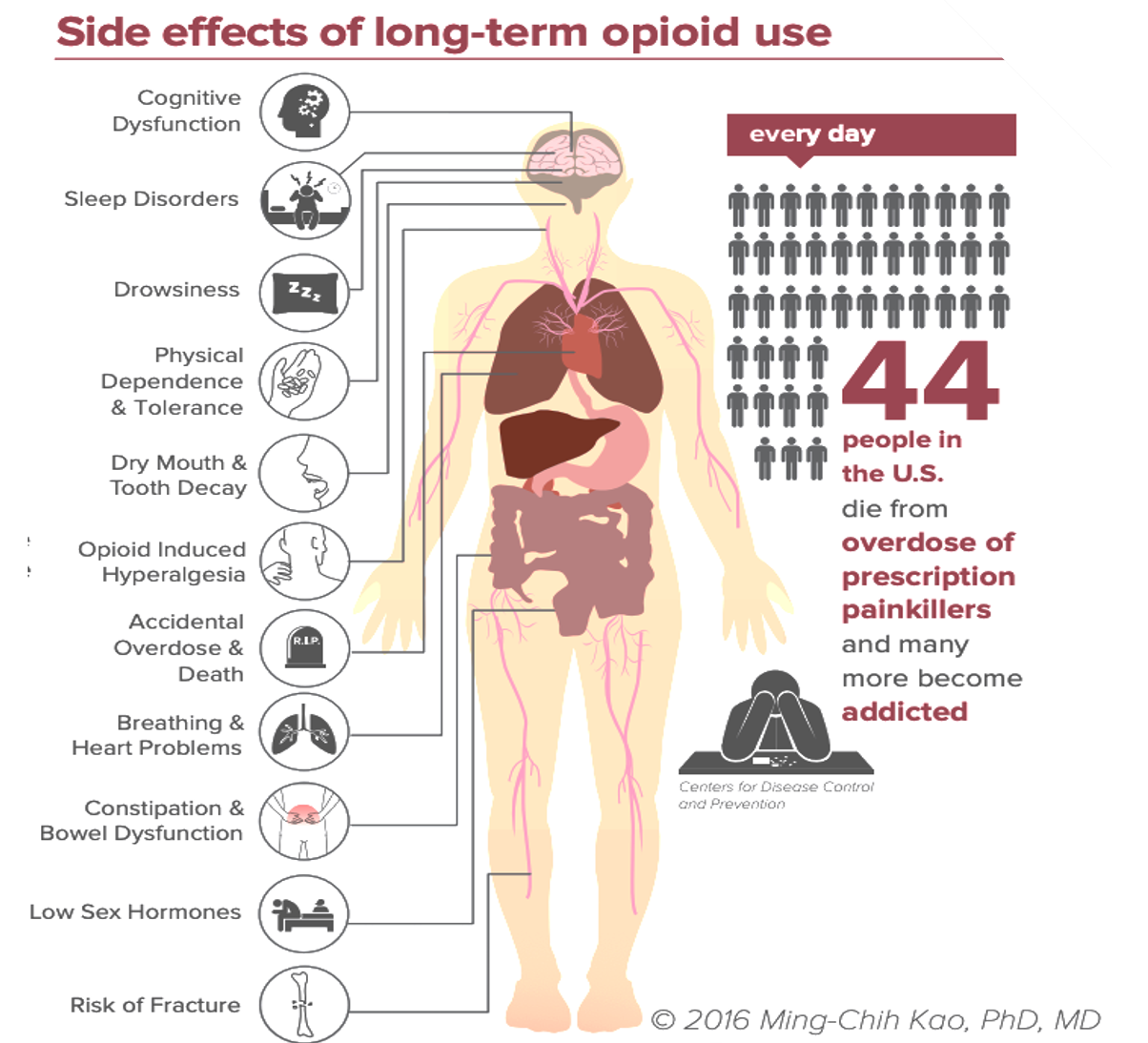
The severity and persistence of the disease combined with inadequate relief and side effects commonly drives patients to opioids.
High Biopharma is Evaluating an Antibody-Based Candidate to Prevent Pain from Trigeminal Neuralgia at the Source
What are Biologics?
Traditional Pharmaceuticals
Traditional pharmaceuticals are chemically synthesized in a lab to generate specific, small molecules that interact with biological targets.
These molecular therapies interact non-specifically and can affect other areas of the body, resulting in unwanted or even dangerous side effects.
They generally act as a “dimmer switch” when interacting with the pharmacological target. Symptoms are reduced but cannot always be eliminated within safe dosages or not at all.
One of the benefits of traditional pharmaceuticals is the ability to make them ingestible as a pill or liquid.
Biologics
Biologics are large and complex molecules produced by cells or bacteria that are comprised of sugars, proteins, and/or nucleic acids, making them highly specific to their physiological targets.
They are able to target specific disease-causing proteins and cells to treat severe conditions like cancer, autoimmune diseases (e.g., rheumatoid arthritis, psoriasis), and chronic infections.
The complexity of biologics prevents them from being taken orally and digested, so they are most commonly administered intravenously (IV) or by injection.
Common biologics are vaccines, Insulin, monoclonal antibodies, gene therapies, blood and cell therapies.
Modern lab technologies allow scientists to create instructions for the cell or organism which produces the biologic of interest that is later isolated and purified.
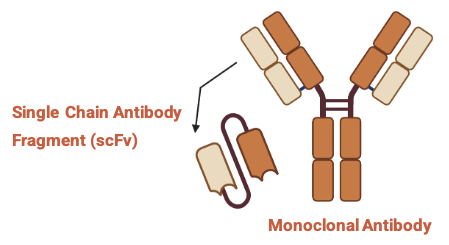
Our Biologic
HBP007 is a single chain antibody fragment (scFv) made specifically to modulate the activity of P2X4, a protein that becomes overexpressed in response to nerve injuries, resulting in neuroinflammation and eventually pain.
This pathway can become stuck in an endless loop that doesn’t allow neuroinflammation to resolve, resulting in chronic neuropathic pain.